
Psychological considerations
- Previous personal experience - the patient may have had an unpleasant experience of having a chest drain inserted previously. 50% reported significant pain on chest drain insertion (BTS)
- Needle phobia - consider cautious administration of a low dose of IV benzodiazepenes.
- Fear - reassure the patient
- Understanding - having too much/too little information
Best Practice Statement
Always give analgesia and consider anxiolytics unless contra-indications
Rationale: Minimise pain and anxiety.
Source of Evidence: BTS guidelines
Patient Education
Communicating and informing the patient of exactly what the procedure involves can reduce anxiety and fears. The patient should be made aware of why he/she is having the procedure, the benefits and the potential complications before obtaining informed consent. Establish if the patient has any known allergies prior to the procedure - the patient may have an allergic reaction to local anaesthetic.
It is important that the patient should know about care of their chest drain, including important safety aspects, however this can normally wait until after the drain has been inserted and will be dealt with after the procedure.
Patient Positioning and site of insertion
Lie patient down if they are able to with the hand of the arm on the side that the drain is going to be inserted into behind the patient's head or held abducted and externally rotated by an assistant.
Chest drains should be inserted through the safe triangle as this minimises risk to surrounding structures (long thoracic nerve, muscle, breast, axillary structures). Insertion through the safe triangle (4th or 5th intercostal spaces in anterior axillary line) also helps to prevent the drain being placed too low with the potentially fatal risks of damage to the liver and spleen.
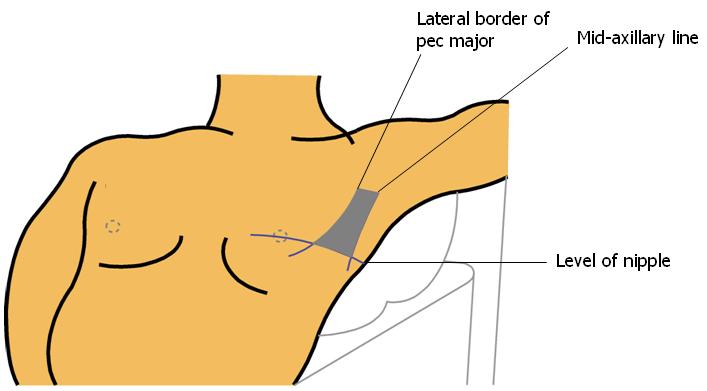
Boundaries of safe triangle are Lateral border of pectoralis major anterior, mid-axillary line posterior, level of nipple inferior.
Griffiths in 2005 noted that 45% of junior doctors chose a point of insertion out with the safe triangle, with 25% choosing a point too low (risks damage to liver and spleen).
Occasionally drains are placed in an anterior or posterior position to access a loculated collection of fluid. This is a specialised procedure and should be performed under ultrasound guidance wherever possible and only by those who are competent in this procedure.
 [D]
[D]Figure 6. Safe triangle
Best Practice Statement
Make sure that the drain is to be inserted through the safe triangle
Rationale: Minimise risk of damage to underlying structures
Source of Evidence: NPSA and BTS guidelines
Patient Safety
The procedure should ALWAYS be carried out in an environment with full resuscitation equipment, including suction. The patient should be monitored, receive oxygen and have an intravenous cannula inserted before the procedure. As well as the competent practitioner who will insert the drain there should be an assistant present who is trained in the care of chest drains AT ALL TIMES. This assistant is required to open packs and equipment so that asepsis is maintained. They are also responsible for monitoring the patient and double-checking safety aspects such as side of insertion. For trainees it is ESSENTIAL to ensure appropriate senior supervision is in place until clinical competence is reached.
Activity
1 |
The boundaries of the safe triangleThe boundaries of the safe triangle are: the lateral border of pectoralis major anterior; the mid-axillary line posterior and the level of nipple inferior. |